Does Your Brain Eat Itself? The Surprising Link to Sleep Deprivation
Written by: David Hernandez
|
Published on
|
Time to read 14 min
If you’ve ever seen the headline “sleep deprivation makes your brain eat itself,” you probably wondered whether that’s sensationalism or science. The reality is more nuanced—and more motivating.
Your brain isn’t gnawing on neurons like a midnight snack, but chronic sleep loss does tip your brain’s house-cleaning systems toward more aggressive “cleanup,” and that can set the stage for inflammation and cognitive decline over time.
Most of us have shrugged off a few late nights without giving much thought to long-term brain health. Let’s unpack what’s really happening, why it matters, and what you can do about it, starting tonight.
The Science Behind Why Your Brain “Eats Itself”
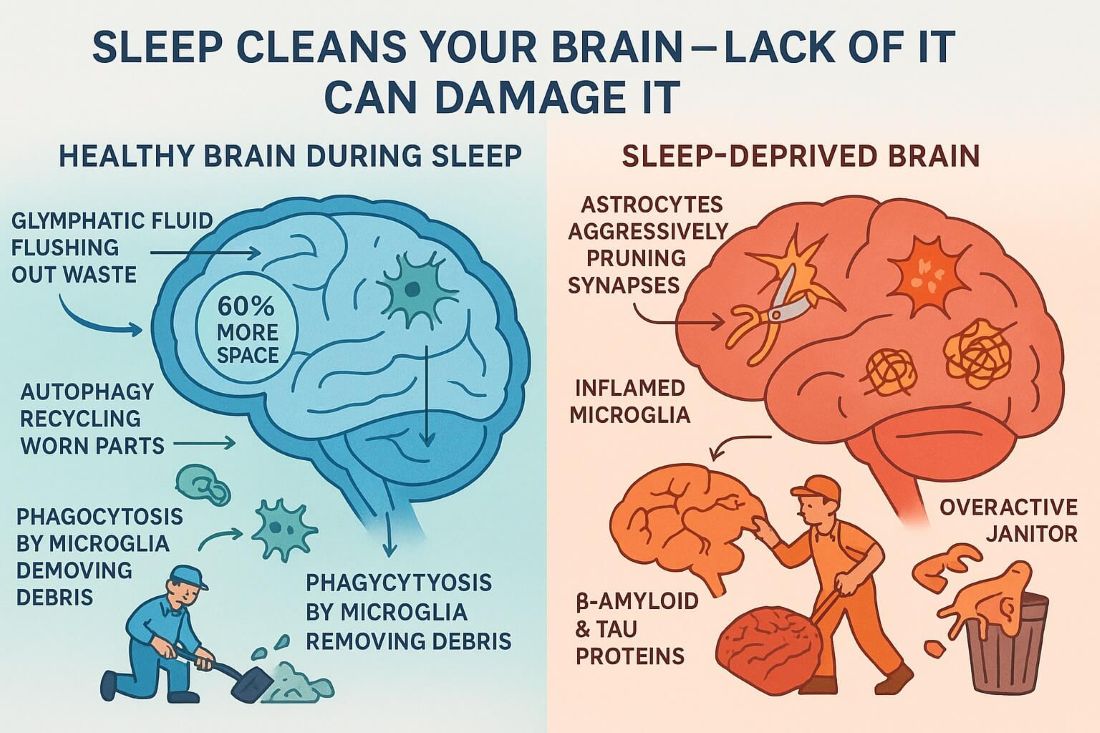
In healthy brains, two forms of cellular cleanup keep things humming:
Autophagy (“self-eating”): cells recycle worn-out parts inside lysosomes—the cell’s recycling centers. It’s a survival and housekeeping process, not self-destruction. (Source: NaturePMC)
Phagocytosis: immune cells (in the brain, microglia) engulf and remove debris, inactive synapses, and dying cells. This sculpts neural circuits during development and clears damage during life (Source: FrontiersPMC)
When you’re chronically short on sleep, these systems change. In a landmark mouse study, researchers kept mice awake and found astrocytes (support cells) ramped up “synaptic pruning”, literally consuming bits of synapses, while microglia showed signs of priming toward a more inflammatory state. Think of it as the night crew switching from light tidying to heavy-duty stripping of your brain’s wiring. (Source: Journal of Neuroscience)
At the same time, deep sleep opens your brain’s glymphatic system, a fluid “rinse cycle” that increases interstitial space by ~60% and clears metabolic waste such as β-amyloid (a protein linked with Alzheimer’s). Less sleep means less nightly clearance. (Source: Science)
Human data connect the dots: a single night of total sleep deprivation raises β-amyloid in brain regions vulnerable to Alzheimer’s, and partial sleep loss increases tau, another protein implicated in neurodegeneration. These aren’t permanent after one rough night, but chronic patterns are concerning. (Source: PNASPubMed)
Bottom line: Your brain isn’t “eating itself” in the cartoon sense, but sleep loss shifts maintenance toward more pruning and less detox, nudging biology in the wrong direction. Picture a janitor who starts aggressively tossing out items that aren’t even trash—this is what happens when your brain overdoes cleanup during sleep loss.
Synaptic balance: The Synaptic Homeostasis Hypothesis proposes that waking strengthens lots of synapses; slow-wave sleep scales them back to keep energy use and noise in check while preserving the most important connections. Evidence supports both pruning and strengthening, depending on circuit and sleep stage. (Source: PubMedPMCFrontiers)
It’s not just about feeling rested. Your brain is literally doing housekeeping that affects how you think, remember, and react the next day.
REM’s role: In animals, REM sleep helps remodel the spine, pruning some and stabilizing others after learning, fine-tuning circuits for the next day. (Source: PMCNature)
Waste clearance: During deep NREM, the glymphatic system flushes metabolites like β-amyloid more efficiently—one reason you feel “clearer” after real sleep. (Source: Science)
In short: sleep recalibrates connectivity and takes out the trash.
Why Sufficient Sleep Is So Important for Brain Health
Missing out on sleep doesn’t just make you tired. It’s like skipping regular oil changes for your brain. From reaction time to long-term brain aging, sleep touches everything.
Cognitive performance: Sleep loss slows psychomotor vigilance (reaction time) and increases attention lapses, one of the most sensitive, well-replicated findings in sleep science. (Source: PMC)
Safety: Drowsy driving contributes to a substantial share of fatal crashes in the U.S.; recent analyses estimate ~18% of fatal crashes involve a drowsy driver. (Source: AAA Foundation for Traffic Safety)
Protein clearance: Regular insufficient sleep blunts the nightly β-amyloid/tau clearance “edge,” nudging risk over years. (Source: PNASPubMed)
Aim for at least 7 hours per night (adults). That’s consistent with major U.S. guidelines and reflects the dose–response relationship between sleep and health outcomes. (Source: AASM)
6 Ways in which Severe Sleep Deprivation Negatively Impacts Your Brain
Severe or sustained sleep loss doesn’t “melt” your brain, but it does push multiple systems—cellular cleanup, protein handling, immune activity, and even brain wiring—into directions that are adaptive in the short term and potentially harmful when repeated.
1. Immediate molecular changes (hours to days)
β-amyloid rises after one all-nighter. In a controlled PET study, healthy adults who stayed awake for ~31 hours showed about a 5% increase in β-amyloid in the hippocampus and thalamus, regions vulnerable early in Alzheimer’s disease. That signal appeared after just one night without sleep. (Source: PNASNational Institutes of Health (NIH)
Tau also surges with sleep loss. Experimental sleep deprivation boosted CSF tau by >50% in humans; in mice, interstitial tau increased ~90% during normal wake and ~100% with sleep deprivation, and chronic deprivation accelerated tau spread across brain regions. Mechanistically, more wake time means more neuronal activity and more tau release into extracellular fluid. (Source: PMCPubMed)
What this means: A single rough night can transiently shift core Alzheimer’s-related proteins in the wrong direction. One night won’t cause disease, but repeating this pattern removes your margin for error. (Source: PMCScienceDirectBioMed Central)
2. Cellular cleanup tilts toward over-pruning (days to weeks)
In mice, astrocytes, the support cells that help remodel synapses, engulfed more synaptic elements after both acute and chronic sleep loss. At the same time, microglia (the brain’s immune cells) showed activation/priming patterns, a shift toward a pro-inflammatory state. Together, that’s “more pruning + more immune readiness,” which is useful during acute stress but worrisome if it becomes the baseline. (Source: The Journal of NeurosciencePubMed)
Why you should care: Normal pruning keeps circuits efficient. Over-pruning can chip away at healthy connections, and microglial priming makes the brain more reactive to subsequent insults (illness, stress, toxins). (Source: The Journal of Neuroscience)
3. Barriers, blood flow, and inflammation (weeks to months)
Blood–brain barrier (BBB) integrity can suffer with prolonged sleep restriction in animal models, leading to hyperpermeability, a leaky gate that admits inflammatory signals and impairs waste clearance. Pericyte dysfunction (cells that help maintain the BBB) has also been observed after repeated deprivation. These shifts create a more inflammatory microenvironment and could hinder nightly “rinse cycles.” (Source: PMC)
Reviews conclude that chronic sleep disturbance is consistently associated with amyloid accumulation, tau pathology, and cognitive decline over time, reinforcing a mechanistic link between poor sleep and neurodegeneration. (Source: PMCScienceDirect)
4. Wiring stress you can see on MRI (days to months)
After 24–32 hours of total sleep deprivation, diffusion MRI studies show widespread changes in white-matter microstructure, signatures consistent with transient edema or altered axonal/glial function. Some changes normalize with recovery sleep, but repeated cycles plausibly add wear-and-tear. (Source: PLOSPubMedPMC)
5. Dose, pattern, and who’s at higher risk
Dose/pattern: Acute total deprivation (e.g., an all-nighter) produces spikes in β-amyloid/tau; chronic partial deprivation (e.g., 5–6 hours/night for weeks) produces cumulative deficits in vigilance and mood and is linked in observational work to higher amyloid burden and faster cognitive decline. The combination—short nights plus circadian disruption (rotating shifts, overnight work)—appears especially unfavorable.
Genetic modifiers:APOE-ε4, the strongest common genetic risk factor for Alzheimer’s disease, seems to synergize with sleep disruption, i.e., poor sleep may have a larger biological “cost” in ε4 carriers, and ε4 itself can worsen sleep architecture, creating a feed-forward loop. (Source: JCIPubMedPMC)
Circadian misalignment: Night- and shift-work cohorts show associations with later-life dementia risk; mechanisms likely include chronic circadian disruption layered atop sleep restriction. (Source: PMC)
6. What recovers—and what might not
The protein spikes (β-amyloid/tau) described above are acute, measured within hours of sleep loss; they can subside with recovery sleep. But recurrent surges, reduced glymphatic clearance, BBB stress, and glial priming together form a biologically plausible path from years of poor sleep to measurable pathology and cognitive decline.
In parallel, imaging suggests many white-matter changes after short-term deprivation are reversible, yet chronic cycles may nudge the system toward maladaptive remodeling. (Source: PMCPubMedPLOS)
The takeaway for you
A single bad week won’t “doom” your brain. But the combination of repeated short nights, circadian disruption, and risk factors (snoring/OSA, APOE-ε4, metabolic disease) raises the stakes. Think of sleep as your brain’s overnight repair crew—cut their hours too often, and things start to fall apart.
The prudent, evidence-aligned move is to treat sleep as preventive brain care—prioritize 7+ hours, fix snoring/possible OSA, and protect your circadian rhythm so your brain’s cleanup crew can restore rather than over-strip. (Source: The Journal of Neuroscience)
How Snoring Affects Sleep Quality and Brain Health
That familiar nighttime buzz might sound harmless, but it could be your brain’s biggest sleep saboteur.
Snoring ranges from benign to a sign of obstructive sleep apnea (OSA), where the airway collapses repeatedly during sleep. People with OSA often snore loudly, then have silent pauses followed by gasps or snorts; sleep becomes fragmented, oxygen dips, and the brain’s nightly maintenance suffers. (Source: AASM)
Snoring is common—estimates include ~45% of adults snoring occasionally and ~25% regularly—but frequent/loud snoring, witnessed apneas, morning headaches, or excessive daytime sleepiness should prompt screening. (Source: Johns Hopkins Medicine)
How to Mitigate the Negative Effects of Poor Sleep on Brain Function (Starting Tonight)
When you’re trying to protect your brain on a tough schedule, quality of sleep matters as much as the amount. Fragmented, noisy, “stop-start” sleep robs you of deep (N3) and REM stages, the very phases tied to memory, mood regulation, and your brain’s nightly waste clearance via the glymphatic system.
Large cohort and clinical studies show that poor sleep quality (and fragmentation) is linked to worse cognitive performance even after accounting for sleep duration; both too little and too much sleep are also associated with cognitive decline, but quality is a distinct, modifiable lever. (Source: PubMedPMCNature)
Mechanistically, deep sleep expands interstitial space and boosts metabolite clearance (including β-amyloid); when sleep is broken by snoring, you get less time in those restorative stages, and clearance suffers. (Source: PMC)
Reduce snoring at the source with a custom, adjustable oral appliance made by VitalSleep
You can’t fix what you don’t notice. So, if your partner complains about your snoring, it might be time to take it seriously.
At VitalSleep we have designed an FDA-cleared, anti-snoring mouthpiece that gently positions your lower jaw forward to help open the airway, reduce vibration of soft tissues, and quiet snoring. By cutting down on arousals and restoring steady airflow, you give your brain a better shot at sustained deep and REM sleep i.e., better sleep efficiency, not just more time in bed.
Why this approach is evidence-based
Oral appliances (MADs) work for primary snoring and many cases of obstructive sleep apnea (OSA). Meta-analyses and guidelines show mandibular advancement devices significantly reduce apnea–hypopnea index (AHI) and snoring; while CPAP is typically stronger physiologically, MADs are effective and appropriate, especially when CPAP isn’t tolerated or in mild–moderate OSA.
Daytime function and sleep quality improve for many users. Evidence briefs from professional bodies report improvements in daytime sleepiness and quality of life, with generally better adherence to oral appliances than CPAP, which is critical for real-world benefits. (Source: American Dental AssociationAADSM)
Recent clinical data link MADs to deeper sleep and patient-reported sleep quality. A 2024 controlled study found two MAD designs both reduced respiratory events; one device improved N3 (slow-wave) sleep and sleep quality while lowering snoring loudness and daytime sleepiness. That’s precisely the “quality” gain your brain needs. (Source: BioMed Central)
Partners sleep better, too. Treating snoring/OSA with oral appliances, CPAP, or surgery improves bedpartner sleep, which often feeds back into healthier household routines (and adherence). (Source: PMCScienceDirect)
Why VitalSleep specifically
FDA-cleared for snoring reduction, made in the USA, with Accu-Adjust micro-titration in ~1 mm increments so you can fine-tune comfort and effect at home. The boil-and-bite fit creates a custom mold for better retention.
How to get the best results (quick start)
Fit carefully (boil-and-bite) and start at a modest advancement; wear for 2–3 nights, then micro-adjust until snoring meaningfully drops while comfort remains high. (Small steps reduce jaw soreness.)
Stack the basics that support nasal airflow: saline rinse before bed if congested; side-sleeping to reduce airway collapse; avoid alcohol within 3–4 hours of bedtime (it relaxes airway muscles and worsens sleep-disordered breathing). (Source: PMC)
Monitor outcomes: Ask your partner about snoring volume/frequency, track daytime alertness, and consider a snoring- or sound-monitoring app for objective feedback. If loud snoring persists, or you have witnessed apneas, morning headaches, or significant daytime sleepiness, book a sleep evaluation to rule out OSA. (Oral appliances help many with OSA, but diagnosis matters.) (Source: Sleep Medicine Resources)
Pair VitalSleep with these high-impact tactics (brain-friendly and practical)
Strategic “coffee nap” for emergencies. Drink ~100–200 mg caffeine, then nap 15–20 minutes; controlled studies in drivers show caffeine, a nap, or both together improve alertness and reduce impairment. Avoid late-day use.
Time caffeine wisely. Most adults can safely consume ≤400 mg/day; the half-life averages ~5 h (range ≈2–12 h), so set an early-afternoon cutoff to protect nighttime sleep.
Morning light + daily movement. Bright light soon after waking anchors your circadian clock; regular exercise improves subjective sleep quality across trials.
“Bank” sleep before short nights; recover after. Pre-loading extra sleep and following with a recovery night can partially restore vigilance.
Avoid alcohol before bed. It fragments sleep and worsens sleep-disordered breathing; higher intake is linked to ~25% higher OSA risk. (Source: PMC)
Small tweaks like these don’t require a total life overhaul. They just make good sleep easier to reach.
Why this matters for brain health (quality and quantity)
Cognition tracks with sleep quality. Poor sleep quality and fragmentation are associated with worse working memory and episodic memory and higher odds of cognitive dysfunction, even after adjusting for sleep duration.
Optimal duration helps when it’s consolidated. Population neuroimaging suggests a non-linear relationship where ~7 hours is associated with the best performance and healthier grey-matter profiles; fragmented sleep undermines these benefits. (Source: Nature)
Physiology explains the link. Deep NREM sleep promotes glymphatic clearance (β-amyloid and other metabolites). Reducing snoring-induced arousals gives you more time in the phases that perform this “rinse cycle.” (Source: PMC)
A quick safety note
VitalSleep is designed and FDA-cleared for snoring reduction. If you snore and have red flags for OSA—witnessed pauses in breathing, gasping, daytime sleepiness, morning headaches, resistant hypertension, or nod-off driving—talk to a clinician about home sleep apnea testing or a lab study.
In short: Tackling snoring with a custom, adjustable mouthpiece like VitalSleep is one of the fastest, most practical ways to upgrade sleep quality tonight, supporting the very brain processes (deep sleep, REM, and glymphatic clearance) that keep you sharp tomorrow and resilient over the long haul.
Sleep Apnea & Brain Health: What It Is, How to Diagnose and Treat It
What is OSA? Repeated episodes of airway collapse cause oxygen drops and arousals from sleep, undercutting deep/REM sleep and nightly brain cleanup. Common symptoms: loud snoring, witnessed pauses, choking/gasping, morning headaches, dry mouth, and daytime sleepiness. Sleep apnea is often undiagnosed, but it can quietly chip away at your focus, mood, and memory over time.
How to diagnose:
Polysomnography (PSG) in a sleep lab is the standard. For many adults at high risk of moderate–severe OSA without major comorbidities, home sleep apnea testing (HSAT) is also appropriate. Your sleep specialist will choose based on your history and risk profile.
If HSAT is negative but symptoms are strong, you’ll typically need in-lab PSG.
Why treatment matters for your brain: Chronic untreated OSA is linked with white-matter and cognitive changes; encouragingly, CPAP can partially reverse white-matter abnormalities and improve cognition over months, underscoring the brain’s capacity to rebound.
Treatment options:
CPAP/PAP (first-line for most).
MADs (especially for mild–moderate OSA or CPAP-intolerant patients). Weight loss interventions (including lifestyle and, for eligible patients, tirzepatide, now FDA-approved for OSA with obesity). (Source: U.S. Food and Drug Administration)
Targeted surgeries or nerve stimulation for select anatomies.
Red flags—seek evaluation: Loud habitual snoring plus witnessed apneas, unrefreshing sleep with daytime sleepiness, morning headaches, refractory hypertension, atrial fibrillation, or significant cognitive fog.
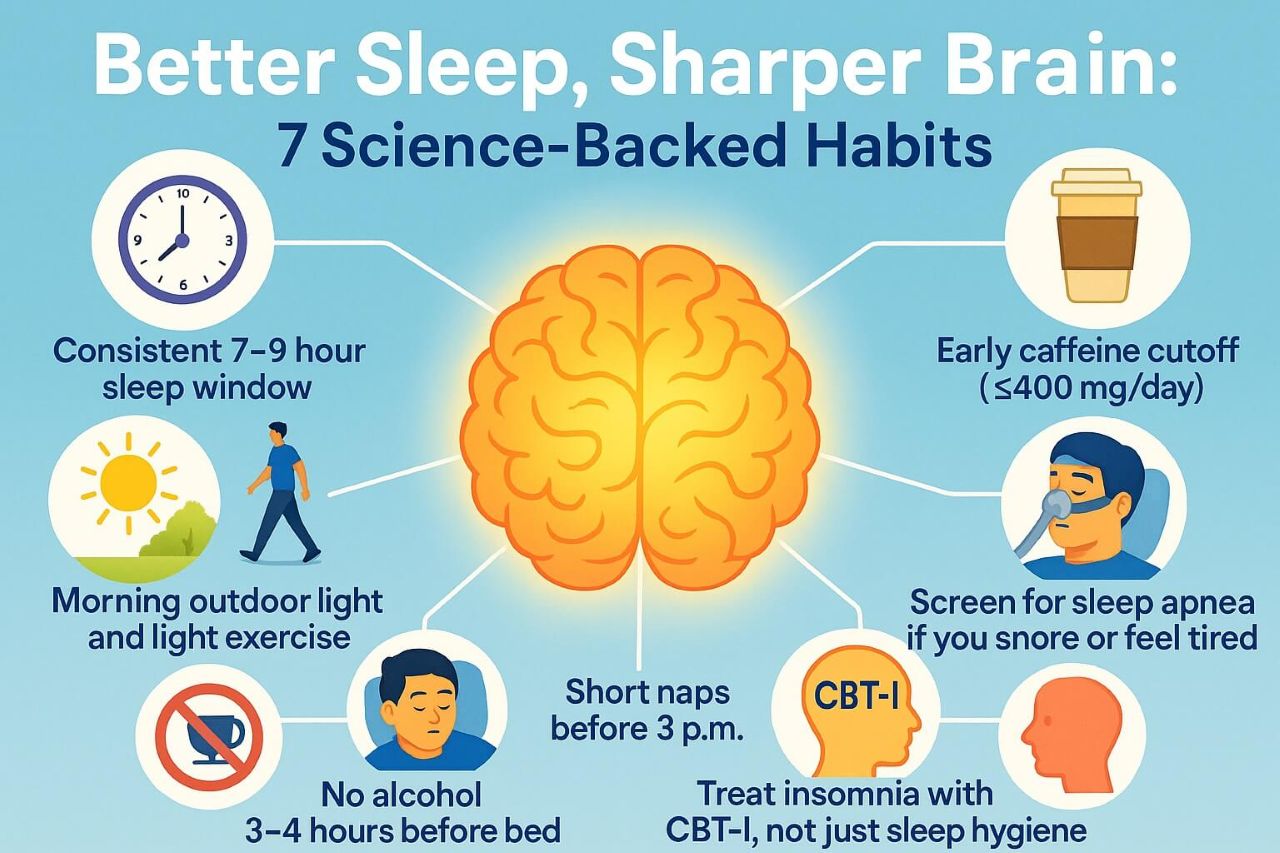
7 Ways to Protect and Improve Brain Health (Sleep-First Edition)
Guard your sleep window. Pick a realistic 7–9 hour window and defend it most nights. Consistency is the scaffold for circadian stability and better sleep depth. (Adults: ≥7 hours recommended.)
Anchor mornings with light and movement. Get outdoor light soon after waking (even on cloudy days) and add a short walk. Morning light helps shift your internal clock earlier; exercise enhances sleep quality.
Keep caffeine early and modest. Max ≤400 mg/day; stop by early afternoon because of caffeine’s long and variable half-life (often ~5 hours, sometimes much longer).
Use naps strategically. If needed, 10–20 minutes before 3 p.m., consider a coffee nap when safety is at stake (e.g., long drives), but don’t let naps replace nighttime sleep.
Limit alcohol within 3–4 hours of bed. It reduces REM, fragments sleep, and increases airway collapsibility, which is especially risky if you snore or have OSA.
Screen for sleep apnea if you snore or feel unrefreshed. Treatment can improve daytime function and may reverse some brain changes linked to OSA.
Treat insomnia with CBT-I, not just “sleep hygiene.”Cognitive Behavioral Therapy for Insomnia is first-line and effective (often delivered via structured programs).
These are the kind of changes your future self will thank you for.
FAQ: Does Your Brain Eat Itself?
1) Does your brain really “eat itself” when you don’t sleep?
Not literally. But chronic sleep loss pushes normal cleanup systems—like astrocytes (which prune synapses) and microglia (which clear debris)—toward overactivity, while reducing the deep-sleep “rinse cycle” that helps remove metabolic waste such as β-amyloid. The result is less restoration and more wear and tear over time.
2) What matters more for brain health—how long I sleep or how well I sleep?
Both. Adults generally need 7+ hours a night, but quality (uninterrupted, consolidated sleep with enough deep and REM) is just as important. Fragmented sleep from snoring or sleep-disordered breathing cuts into deep/REM sleep, which is linked to memory consolidation, mood regulation, and glymphatic clearance. Reducing snoring improves sleep efficiency, the percentage of time in bed you actually spend asleep.
3) How do I know if my snoring is just annoying or a health risk?
Red flags include: loud nightly snoring, witnessed pauses in breathing, choking/gasping at night, morning headaches, dry mouth, and excessive daytime sleepiness. High blood pressure, atrial fibrillation, and nod-off driving increase concern. If these apply, ask your clinician about screening and a home sleep apnea test or in-lab study.
4) Will an anti-snoring mouthpiece like VitalSleep actually help?
Yes, mandibular advancement devices (MADs) are a well-studied option. By gently advancing the lower jaw, they open the airway, reduce tissue vibration, and lower snoring frequency and loudness. For many people with primary snoring(and even some with mild–moderate OSA), MADs improve symptoms and sleep quality; CPAP is usually more potent for moderate–severe OSA, but MADs are often easier to stick with. Adherence matters in the real world.
5) How fast will I notice benefits with VitalSleep?
Most users notice changes within the first 1–2 weeks after proper boil-and-bite fitting and a few small adjustments. Look for fewer awakenings, less morning grogginess, and partner-reported quieter nights. Tracking with a snoring or sound-monitoring app can make improvements obvious.
6) Are there side effects or reasons I shouldn’t use a snoring mouthpiece?
Common, usually temporary effects include jaw or tooth soreness, extra salivation, or dry mouth while you acclimate. Go “low and slow” with advancement adjustments and give it several nights between changes. People with loose teeth, active gum disease, significant TMJ pain, or recent major dental work should talk to a dentist first.
7) Can better sleep quality really protect my brain even if my total sleep time doesn’t change much?
Improving quality (fewer arousals, steadier airflow, more deep/REM) is strongly associated with clearer thinking, better mood, and next-day performance. Because deep sleep supports glymphatic clearance, quieter, less fragmented nights are a practical way to support long-term brain health, independent of just “more hours in bed.”
8) Is one bad week of sleep going to cause permanent damage?
One rough week isn’t destiny. Studies show short-term sleep loss can temporarily raise brain proteins like β-amyloid or tau and impair attention, but recovery sleep improves vigilance and symptoms. The risk comes from repeated sleep fragmentation and chronic short sleep. That’s why tackling snoring now is a smart preventive move. One all-nighter isn’t the end of the world, but repeated bad nights add up fast.
9) What habits amplify the benefits of VitalSleep?
Side-sleeping (use a pillow or bumper to stay off your back)
Alcohol cutoff 3–4 hours before bed (alcohol worsens snoring and fragments sleep)
Nasal care (saline rinse or decongestant use as directed when congested)
Consistent sleep window and morning light exposure
Weight management and regular exercise (both reduce snoring/OSA severity)
10) When should I stop DIY and see a sleep specialist?
If you have witnessed apneas, severe daytime sleepiness, morning headaches, high blood pressure, or heart rhythm issues; are pregnant; or are a commercial driver—or if snoring persists despite a mouthpiece—book an evaluation. Oral appliances, CPAP, positional therapy, and weight-loss interventions are all effective tools; the right choice depends on your diagnosis and severity.
David Hernandez
David is the founder of VitalSleep.com. David has been helping his customers with their snoring issues since 2009.